Theraputic Massage...big fat ouch!!
Okay, normally a massage is nice and relaxing but theraputic massage is a whole different kettle of fish! First...it hurts like a mother! It hurts to get it done and it hurts after.
There are different types of massage so people with FMS should be careful when they go to a massage session.
Thanks to Wikipedia for the information.
Types of massage
There are well over 150 types of massage therapy. Various styles of massage have developed from a number of sources.
Barefoot Deep Tissue
Barefoot Deep Tissue is a blend of Eastern barefoot techniques with Western manual medicine. Clients are typically loosely clothed and lain on floor mat in supine, prone and side-lying positions with pillows or bolsters. No oil is used. Sessions may last 2 minutes or well over an hour. Because the therapist can apply a broad range of pressure with ease and does not have to strain, more effort and concentration can be used to sense and manipulate tissue, release fascia, as well as search for and attack trigger points and other problems, regardless of client's size or build. John Harris, the proceleusmatic mentor who worked in the 1984 Olympics and developed this modality, states that the combination offers a potent new tool for powerfully satisfying, effective deep tissue massage and Trigger Point work regardless of client's size or build. Mr. Harris and Fred Kenyon wrote Fix Pain in 2002, and have been hired by Human Kinetics to write a trade publication with DVD for elite athletes.
Bowen therapy
For more details on this topic, see Bowen Technique.
Bowen Technique involves a rolling type movement over fascia, muscles, ligaments, tendons and joints.
Breema
Breema bodywork is performed on the floor with the recipient fully clothed. It consists of rhythmical and gentle leans and stretches which leads to deep relaxation, increased vitality, and stimulation of the self-healing processes of the body. Sessions can be any length of time, although 50 minutes is common. There are also self-Breema exercises. The essence of Breema is expressed in the Nine Principles of Harmony. The Breema Center is located in Oakland, California, and there are Breema practitioners and instructors in many locations around the world.
Chair massage
Chair massage, also known as Corporate Massage, is by far the most convenient method of massage therapy. A chair massage session typically lasts 12-24 minutes, and is performed while fully clothed. Chair massage promotes better circulation, muscle stimulation and stress relief. This form of massage reduces tension in the back, neck, shoulders, head, arms, hands, legs or feet, providing a deep relaxation effect.
Chair massages are also advantageous because chair massage practitioners will frequently make work- or housecalls. Chair massage can also be done in hotels, airports and convention centers.
Chinese Tui Na massage
For more details on this topic, see Tui Na.
Tui Na is a form of Chinese massage that is similar to Zhi Ya, but focusing more on pushing, stretching and kneading the muscle.
Chinese Zhi Ya massage
Zhi Ya is a form of Chinese massage based on acupressure. It is similar to Tui Na massage except it focuses more on pinching and pressing at acupressure points.
Deep muscle therapy
Deep muscle therapy (created by Therese Pfrimmer), is a massage technique that focuses on using a very specific set of movements applied to all muscles and concentrating on all layers of the muscle that have become depleted of their regular blood and lymphatic flow. This technique aims to restore the circulation with its healing properties to the cellular level. Deep muscle therapy is widely used to treat the following ailments: carpal tunnel syndrome, neck and back pain, headaches, poor circulation, whiplash, and more.
Deep tissue massage
Deep tissue techniques are generally designed for more focused massage work. Working a specific joint, muscle or muscle group, the practitioner can access deeper layers of the soft tissue. Starting superficially and easing into the depth of the muscle slowly often allows more movement. This is the recommended approach in this modality since each person experiences pressure differently. If the pressure is applied too deeply or too quickly, the muscle may tighten to protect that area, and unnecessary damage or inflammation can be induced. Very little lubricant is used as the pressure doesn't travel much over the skin.
The most commonly used 'tools' during deep tissue massage may include, 3 and 6 fingers, reinforced fingers, a flat elbow, opposing thumbs, the heel of the hand or foot, and the forearm. See also: Myofascial Release
Effleurage
Effleurage (from the French effleurer, 'to skim over') consists of long, flowing or gliding strokes, performed with open hands. In many massage sessions, effleurage is used as the initial type of stroking, as it has a calming effect when performed slowly. Effleurage is usually performed in the direction of the heart to promote circulation and lymphatic drainage.
Erotic massage
Erotic massage is a form of massage that includes the genitals and leads to sexual arousal and (sometimes) orgasm. Widely practiced by couples as part of lovemaking. Also sometimes practiced commercially, which may be illegal in some jurisdictions. See also Tantramassage.
Esalen Massage
The basis of Esalen Massage is traditional massage, which works in a very precise manner on the muscle and circulation systems. This is combined with the bodywork approach developed by Charlotte Selver, which emphasizes the deeply relaxing and emotional responses of the body when a conscious, structured and pleasant touch is applied. In addition, gentle rocking of the body, passive joint exercises and deep structural work on the muscles and joints, together with an energetic balancing of the body, are all part of this Esalen Massage “experience”.
Foot or sole massage
Foot massage, as practiced by the Chinese is performed in the context of chi, in that each spot on the sole of the foot corresponds to an internal organ, and the applied therapy is healing to one's overall well being. The theory supposes that an ailment of an internal organ will be associated with the nerve ending on the sole of the foot.
Before the massage, the patient's feet are soaked for about ten minutes in a foot bath, typically a dark colored solution of hot water and Chinese herbs. The massage therapist uses liberal amounts of medicated cream, to moisturize the foot and to provide lubrication. The knuckles on the therapist's hand are usually used to provide a hard and smooth implement for the massage. As pressure is applied to the sole, theory holds that a healthy patient should not feel any strong pain. Painful spots, reflexologists believe, reflect illnesses of other parts of the body. The practitioner rubs and massages the painful spots to break down rough spots and accumulated crystals and increase circulation.
The ailments are healed when the sore spots of the sole are treated and removed by massage. Based on this theory, some shoe liners are made with pressure points to stimulate the soles of the feet to promote better health of the overall body. The nature of these "crystals" has yet to be elucidated or demonstrated scientifically. Regardless of the actual correlation of reflexology to internal organs, many enjoy it for the mix of stimulation and relaxation.
Lomilomi — Traditional Hawaiian Massage
Lomilomi massage is an ancient art from the Hawaiian healing specialists. They were taught their art over 20 years and received their last instructions from their master on his death bed. There are hundreds of styles of Lomilomi, the main ones being the style of Big Island which was passed on by Aunty Margaret Machado, and Maui style from Uncle Kalua Kaiahua. On the island of Kaua'i, Kahu Abraham passed on what is today called Kahuna Bodywork. It is not clear if other current practices - temple style, lomi lomi nui and others - are from Native Hawaiian practitioners or are modern adaptations.
MA-URI massage
MA-URI is a new form of massage introduced by Hemi Hoani Fox in 1990, who cites as its roots Hawaiian Lomi-Lomi Nui dance, claiming increased so-called energy flow within the body and mind. Focus is internal, upon breathing, intent, and concentration. Claimed benefits include mental and physical health. Study and advocation is primarily carried out at the MA-URI Institute, headed by Hemi and Katja Fox. It is currently difficult to find practitioners, though this may change as it grows more popular.
Muscle Energy Technique (MET)
Reciprocal Inhibition (RI) is when the therapist uses a client’s muscle to stretch the opposing muscle. The therapist takes the muscle that they are wishing to stretch to its point of bind. The therapist then gets the client to use the opposing muscle by moving away from the therapist. When the client relaxes the therapist then moves the muscle to realign the muscle fibres therefore stretching the muscle.
As an example, Muscle Energy Technique (MET) Reciprocal Inhibition (RI) can be applied to the calf when the client is lying supine on the treatment couch. The masseur can place one hand on the tibia just below the knee to isolate the knee preventing it from moving. The other hand is placed around the heel so that the masseurs forearm can be used to dorsiflex the foot. This is one of the techniques used by sports massage therapists.
Myofascial Release
Myofascial Release refers to the manual massage technique for stretching the fascia and releasing bonds between fascia and integument, muscles, and bones, with the goal of eliminating pain, increasing range of motion and balancing the body. Injuries, stress, trauma, overuse and poor posture can cause restriction to fascia. Myofascial release frees fascial restrictions, and allow the muscles to move efficiently. This is usually done by applying shear, compression or tension in various directions, or by skin rolling. This is one of the techniques used by sports massage therapists and physical therapists. Myofascial release originators come from Physical Therapy and from Structural Integration (Rolfing); its current developers include John Barnes PT from a Physical Therapy background, and from a Rolfing or Structural Integration background, Art Riggs, Michael Stanborough, Tom Myers, Til Luchau, and others.
Myoskeletal alignment technique
Myoskeletal Alignment Technique (MAT) identifies postural distortions to improve and prevent pain conditions. Proprioceptive Neuromuscular Facilitation (PNF) and myofacial techniques are used to lengthen tight/facilitated muscles while fiber activation techniques tone weak/inhibited muscles. MAT was developed by Erik Dalton.
Neuromuscular therapy
Neuromuscular Therapy (NMT) is used for pain relief and specific problems. Structural and postural imbalances are identified through an initial postural assessment. These are then addressed through systematic and site specific massage. NMT reduces pain, tension, postural imbalance, and lengthens and strengthens tissues. NMT was developed by Paul St. John.
Petrissage
Petrissage (from the French petrir, 'to knead') is one of the five basic strokes of a Swedish massage. It is performed with kneading movement with the whole palm or finger tips, wringing, skin rolling, compress and lifting. Petrissage is usually applied vertically to the muscle tissue.
The benefits include the warming of tissue for deeper work, increase circulation, increase the supply of nutrients and oxygen to muscle, softens superficial fascia, decreases muscle tension, and restoring mobility by decreasing adhesion.
Scalp massage
In some barber shops in Hong Kong, scalp massage often lasts 30 minutes to 45 minutes during shampooing of the hair. It is also very common in India, after applying oil on the hair.
Shiatsu
Shiatsu is a form of Japanese massage that uses thumb pressure and workes along the energy meridians in the body also with a lot of streches the same meridians as acupressure. You are worked on fully clothed on a mat on the floor. It is uncertain whether it originated from Chinese Zhi Ya.
Soft Tissue Therapy
The Assessment, Treatment and Management of Soft Tissue Injury, Pain and Dysfunction. Treatment techniques include:
Trigger point therapy for the alleviation of trigger points.
Myofascial (muscle and fascia) therapy for flexibility/mobility of the connective tissues of our body, or for alleviating fibrous adhesions and decreasing the severity of scars.
Broad handed techniques for reducing swelling or inflammation
Frictions for the ridding of adhesions between fascial layers, muscles, compartments and the like. Frictions also promote healing in tendon pathologies as well as decreasing pain perception.
Sustained pressure (digital pressures) to alleviate hypertonic (tight)areas within muscle and fascia
Other techniques such as Active Release Therapies, Myofascial Release and deep tissue massage are all derivatives of the techniques above. They are NOT unique techniques with unique results.
Stretching - static, dynamic, and/or PNF stretches (proprioceptive neuromuscular facilitation)
Muscle Energy Technique (MET)
Exercise Prescription
Advice:
This is one of the techniques used by sports massage therapists.
Stone massage
Massage in which hot or cold stones, usually basalt or marble, are used to massage the body. Often the stones are placed on key energy points, such as Chakras or meridians, in order to improve energy flow and healing.
Structural muscular balancing
A gentle and effective technique that releases chronic contraction in the muscles. The nervous system is triggered to release contractions through compression applied to muscles placed in a shortened position.
Swedish massage
This style utilizes long, flowing strokes, often but not necessarily in the direction of the heart.Swedish massage is designed to increase circulation and blood flow. There are six basic strokes:effleurage,petrissage,friction,tapotement,compression and vibration.Oil, cream, or lotion is applied on the skin to reduce friction and allow smooth strokes. This style of massage is generally attributed to the Swedish fencing master and gymnastics teacher Pehr Henrik Ling (1776-1839).However, it was in fact the Dutch practitioner Johan Georg Mezger (1838-1909) who adopted the French names to denote the basic strokes under which he systemized massage as we know it today, as Swedish or classic massage. Somehow, the term Swedish Movement System was transposed to Swedish Massage System sometime during the second half of the 19th century. Ling’s system was the Swedish Movement System or Swedish Gymnastic Movement System. This may be how he has become incorrectly associated for so long with Swedish massage. In Sweden, the term "Swedish massage" is not used.
Tai Ji Massage (Tai Chi Massage)
Tai Ji / Tai Chi Massage is massage using the natural principles of Tai Ji, Yin and Yang to achieve balance in the energies of the body, leading to a healthy mind body and spirit.
Tai Ji / Tai Chi The traditional Chinese term refers to the Dao, which is the inexpressible oneness and connectedness of all things. This is inexpressibility of Tao is referred to by Lao Tzu:
Chapter 32
"The Tao is constantly nameless….
As soon as we start to establish a system we have names.
And as soon as there set names,
Then you must also know that it's time to stop"
Te Tao Ching
Translation by Robert G. Hendricks. Ballantine books 1989
Qi/ Chi: This is the linking element material and spiritual (Jing and Shen), or in health terms mind and body.
Chinese medicine is often able to treat sicknesses and problems which are difficult to treat by western medicine by virtue of the fact that they consider the state of the Chi to be an important factor in diagnosis.
Qi Field theory: Qi appears as a field. In order for a sickness to become chronic an integral Qi field establishes itself in the body of the host. The shape and size of this field is variable and can stretch from head to toes in some cases.
Tai Ji Massage Qi Diagnosis: Tai Ji Massage is a Qi treatment and it makes a treatment in terms of Qi. The master practitioner can sense the Qi blockages inside the body and the relationship which they have to each other.
Qi blockages can be a way of getting insight into causes of chronic sicknesses, recurring sicknesses, psychosomatic sicknesses, future sicknesses.
The main use of this techniques is, relaxation and self-exploration, and in a therapeutic way, funtional organ problems, chronic sicknesses and psychosomatic sicknesses.
Tai Ji Massage was developed by Richard Wickes, Li Cun De.
Tantramassage (Tantric massage)
Original Tantramassage is a new form of massage developed in the early 1980s by Andro, Andreas Rothe an experienced Tantra and Bodywork Teacher in Berlin, Germany. The method includes various massage techniques, elements from Bioenergetic, Yoga and Sexualtherapy. The word "Tantra" emphasizes the connection with the old Indian cultural background where the body is seen as the temple of the soul. Clients are in a passive role, supported by breathing techniques they experience a very deep and intense journey through their own body. Every Massage session lasts 90 Minutes or longer. The Tantramassage movement is very popular in Germany and Switzerland, some practitioners are organized in the Association of Tantramassage in Germany.
Thai massage
Known in Thailand as นวดแผนโบราณ (Nuat phaen boran), IPA which correctly translates only as ancient massage or traditional massage, this form of massage is also known as Thai ancient massage, traditional Thai massage, Thai yoga massage, yoga massage, Thai classical massage, Thai bodywork, passive yoga or assisted yoga. It is usually soothing because of its emphasis on stretching and loosening the body. Its roots go back far into history, originating in India based on the Ayurveda, and then becoming popular in Thailand.
Originating in India and drawing from Ayurveda, it has inevitably incorporated modalities like yoga. The receiver is put into many yoga like positions during the course of the massage. In the northeren style there are a lot of stretching movements unlike the southern style where pressure is emphasised. It was believed that the massage art was brought over to Thailand by Shivago Komarpaj (Jivaka Kumarabhacca), a contemporary of Buddha almost about 2500 years ago.
The massage recipient changes into pajamas and lies on a mat or firm mattress on the floor. (It can be done solo or in a group of a dozen or so patients in the same large room). The massage giver leans on the recipient's body using hands and forearms to apply firm rhythmic pressure to almost every part of the taker's body. The massage generally follows the Sen lines on the body-somewhat analogous to Chinese Meridians and Indian nadis. In some gestures, legs and feet of the giver are used to fixate the body or limbs of the recipient. In other gestures, hands fixate the body, while the feet do the massaging action. Usually no oil is applied. A full course of Thai massage typically lasts two hours or more, and includes pulling fingers, toes, ears etc., cracking the knuckles, walking on the recipient's back, arching the recipient's back in a rolling action etc. There is a standard procedure and rhythm to the massage. Sometimes in a large group massage, the practitioners do the procedures in unison.
Note: The traditional therapeutic practice of Thai massage should not be confused with the sexual service of the same name that is available in some hotels and brothels.
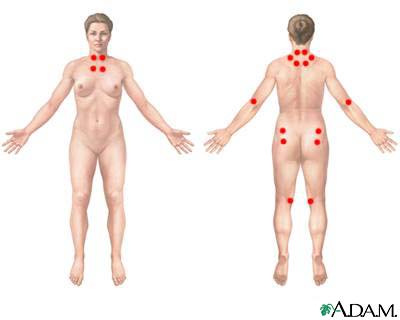
Trigger point therapy
A trigger point is an area of a muscle (about 50 cells) that may refer pain sensations to other parts of the body. Trigger Point Therapy applies manual pressure, or CO2 injections, to these points. With the proper pressure, duration and location, immediate release of tension and improved muscular functioning may occur. This therapy has been known to diminish migraine pain, mock sciatica, mock carpal tunnel syndrome and other pain syndromes, and other symptoms that may have been misdiagnosed. This work is based upon the trigger point research and manuals of Dr. Janet Travell, President Kennedy's physician.
Sometimes this work is incorporated into other styles of massage therapy such as neuromuscular therapy (NMT) or even Swedish
posted by Wendy at 8:15 AM
![]()
![]()